This page will take you through the process of preparation for colonoscopy at the Southwest Endoscopy Center. It contains useful information for "first timers" and for returning patients. Please call us if you have any questions or require any additional assistance.
Our goal is to provide you with a safe, comfortable and accurate examination, and if necessary, to provide you with whatever endoscopic treatment is indicated on the basis of our findings.
|
Watch a funny video
Ms. Butt Meddler presents
Dr. Patricia Raymond
Gastroenterologist
Chesapeake, VA
|
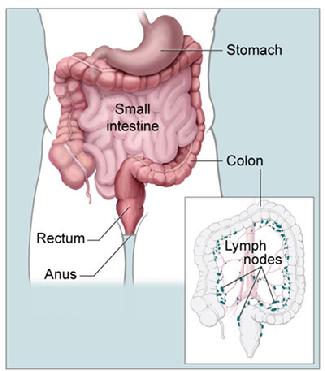 |
| Anatomy of the colon (from the National Cancer Institute) |
|
|
|
What is colonoscopy?
Colonoscopy is an examination of the colon, also called the large intestine, which is the last 5-6 feet of the intestinal tract, ending in the rectum. The examination is performed with a long flexible and steerable tube (colonoscope) which is about the diameter of a finger. The tip of the tube lights the interior of the colon and projects a color image on high definition video monitors. A variety of instruments may be passed through the colonoscope, allowing the doctor to sample tissue, remove small growths, and perform a variety of treatments.
What is a high-quality colonoscopy? (click for more information)
What is an "open access" colonoscopy?
Many patients who are thinking about having a colonoscopy performed prefer to avoid a traditional doctor's office visit with the gastroenterologist prior to scheduling their procedure. Office visits provide an excellent opportunity to meet face-to-face with the doctor and talk in detail about the procedure, but they are also costly and time consuming, and require time away from work and other life activities that many people don't wish to spare.
In some cases the information that a patient and doctor needs to prepare for the safe and effective performance of an endoscopy can be obtained in other ways. Our "open access" program is designed with your easy access in mind. Our experienced registered nurses obtain your health history through a convenient telephone interview process at which time they will answer any questions you have about the planned procedure. The information you provide is entered into your permanent Digestive Health electronic medical record and forwarded to the physician for final review and approval in advance of your procedure date. The forms needed for registration at the time of your procedure are available here.
We are able to offer open access services at this time on a limited case-by-case basis. In some instances an "open access" procedure is not the best option. Either the patient or the doctor may decide that an office visit before scheduling the procedure is the best way to go. Open access services are not a covered benefit of the Medicare program.
I feel fine. Why is my primary care doctor making me go for a colonoscopy?
Colon cancer is the concern. Unfortunately it is a common killer, representing the second leading cause of cancer-related death. Most people with early colon cancer feel perfectly well. Fortunately though, early colon cancer can be detected by colonoscopy at early stages, before it has spread outside the colon. Early stage colon cancer is often highly curable. More importantly, the common growths (polyps) from which most colon cancers may slowly arise (colonic adenomas, or adenomatous polyps) can be detected and removed during a colonoscopy, resulting in the potential prevention of colon cancer. Experts believe that colon cancer deaths may be up to 90% preventable by regular colonoscopy, and that colon cancer itself may be up to 70% preventable.
All individuals should undergo colon cancer screening at or before the age of 50.
Where should I schedule my procedure? (click for more information)
Our doctors perform colonoscopy in Durango at the Southwest Endoscopy Center and at Mercy Regional Medical Center's endoscopy center, which is located in the outpatient surgical area.
I have a family history of colon cancer. When should I get checked?
While most cases of colon cancer occur in people with no familial risk factors, individuals who have a close relative who has had colon cancer, particularly at a young age, are at increased risk themselves for developing colon cancer. They should be initially examined at a younger age, and examined more often, than individuals without risk factors. A familial risk is also conferred when close relatives have had common benign colon polyps (adenomas), particularly when the polyps have occurred at a young age, have occurred in large numbers or have been "advanced" under the microscope or large in size, such as those requiring surgical rather than endoscopic removal.
When doctors ask about a family history of colon cancer or colon polyps we want to know how many blood relatives have had these diagnoses, at what age, and how close the relative was or is to the patient. Relatives are commonly described as "first-degree" (meaning a parent, sibling or child), "second-degree" (meaning grandparent, aunt, uncle, niece or nephew) or "third-degree (meaning great-grandparent or first cousin).
About one out of every four patients in whom colon cancer is diagnosed have a family history of colon cancer. In 16-20% of cases the affected family member is a first-degree relative. Studies show that having a family history of colon cancer increases the risk of developing the disease in the following manner:
-
general population: 6% lifetime risk
-
third-degree relative: 7% lifetime risk
-
second-degree relative: 8% lifetime risk
-
first-degree relative who developed cancer at age > 50: 12% lifetime risk
-
first-degree relative who developed cancer at age < 50: 22% lifetime risk
-
two first-degree relatives: 30%
There are a few uncommon but well-defined familial genetic colon cancer syndromes in which many relatives develop colon cancer at very young ages. Hereditary non-polyposis colon cancer (HNPCC, Lynch syndrome) and familial adenomatous polyposis (FAP) are examples. If these syndromes are suspected you will need to discuss your family and personal history with us in detail and we will discuss referral for genetic testing with you.
In general, we recommend that individuals with a family history of colon cancer be classified and screened as follows:
-
high risk (first-degree relative with colon cancer or polyp diagnosed at age < 60, or two first-degree relatives diagnosed at any age): colonoscopy at age 40 or 10 years younger than the earliest diagnosis, whichever is earliest; repeat at 5 year intervals
-
some increased risk (first-degree relative with colon cancer or colon polyp at age > 60, or two or more second-degree relatives with colon cancer: colonoscopy at age 40
We understand that it is distressing to live with the knowledge that you have an increased statistical risk of developing a serious and potentially fatal disease such as colon cancer. However, there is good news. Regular colonoscopy can dramatically reduce the probability that you will develop colon cancer. Recent studies also show a new "silver lining" related to colon cancer family history. While having a family history of colon cancer does increase your chance of developing the disease, it also is associated with a decreased risk of cancer recurrence and cancer-related death, compared to individuals who have colon cancer but no family history, when an advanced colon cancer occurs and is being treated with chemotherapy.
I've heard that the "colon cleanse" is the worst part of the procedure. What should I expect? What can I do to make it easier?
A clean colon is essential for a safe and effective colonoscopy. If the doctor encounters residual waste material during a colonoscopy it may be necessary to stop the procedure before it is completed, and retained waste may hide serious problems, such as flat polyps or cancers.
Gastroenterologists use a variety of methods and products to cleanse the colon of all waste prior to a colonoscopy examination. Our preferred cleansing program uses a 4 liter (approximately 1 gallon) slightly salty-tasting fluid which is taken orally and passes all of the way through the gastrointestinal tract, resulting in diarrhea which becomes increasingly clear, and ultimately takes on the appearance of urine. This fluid is a prescription product which is typically furnished as a powder in a 1 gallon plastic jug, to which water must be added prior to beginning the cleansing procedure. Some products contain optional flavor packs which may make the "prep" more tolerable. Many patients have found that having a few wedges of lime nearby can also help, serving as something to suck on at the completion of each glass of solution, which helps cut the salty flavor. Using a straw may also help. Placing the straw tip as far back into your mouth as possible allows the fluid to "bypass" many of your taste buds. Swishing diluted flavored soda pop in your mouth, and then spitting, after each glass may also help. Moist anal cleansing wipes (Preparation H Medicated Wipes or similar generic products) can make the later stages of the prep much easier.
The product provided often depends on what the pharmacist has available or what your insurer may allow. A generic preparation (PEG-3350 and electrolytes for oral solution) is often dispensed. Common brand named products include GoLytely®, NuLytely® and CoLyte®.
Our standard preparation instructions allow for consumption of regular food (avoiding fruits and vegetables containing seeds and fibrous foods) until about 6:00 p.m. of the evening prior to examination, after which only "clear liquids" are allowed until your procedure is completed. At about 6:00 p.m. you will begin drinking the prep solution. You will need to drink half of the jug (2 liters) in less than 2 hours. You will then take two laxative tablets (bisacodyl 5 mg). The remaining liquid prep should be refrigerated and must be consumed the following morning, over less than two hours, such that all oral intake is completed at least 2 hours prior to your arrival at our facility. It is very important from the standpoint of sedation safety that you have absolutely nothing by mouth (NPO in medical terminology) for at least 2 hours prior to your procedure.
While individuals respond to the preparation differently, most will develop a feeling of fullness, bloating and distension after drinking a few glasses. Some people even report that they feel as if they will explode! Occasionally, vomiting occurs. While these symptoms are unpleasant, it is important to try to stay on course with your drinking. Generally within 1-3 hours after starting the prep solution a bowel movement will occur and the sensation of distension will ease. Diarrhea may rapidly follow. You should plan to stay near a toilet until the frequency of your bathroom visits slows down. Most patients can get a few hours of sleep, though some will be kept up by diarrhea. Your body's response to drinking the evening dose of solution may guide you with respect to how early you need to start your morning cleansing, and what to allow with regard to driving time and planning restroom availability during transportation to our facility.
While we believe that our standard preparation generally provides the safest, best tolerated and most reliably effective cleansing available, some individuals have difficulty tolerating such large volumes of fluids. Based on your medical history, intermediate volume liquid preps (HalfLytely®, MoviPrep®, SUPREP®, Prepopik™) or tablet-based cleansing preparations (Visicol®, OsmoPrep®), may be appropriate. A popular over-the-counter option, the MiraLAX/Gatorade prep, is another option for some patients.
Potentially serious kidney problems (acute nephrocalcinosis leading to the need for dialysis and renal transplantation) and electrolyte abnormalities (with related cardiac rhythm irregularities) may result from bowel cleansing for colonoscopy with phospho-soda. At Digestive Health we discontinued the routine use of phospho-soda (nonprescription Fleet® Phospho-soda, generic phospho-soda, Visicol®, OsmoPrep®) for colonoscopy cleansing in November 2005. The FDA issued an alert on December 11, 2008 warning of the risk associated with the use of these agents. The C.B. Fleet company responded immediately by issuing a voluntary recall of their over-the-counter Phospho-Soda products and asked healthcare professionals to cease the use of these products for bowel cleansing prior to colonoscopy.
Medical Literature Search: Phospho-soda problems
What happens after I arrive and check in?
Once you've completed the cleansing preparation the rest of the procedure is generally easy. You will need to check in at least 45 minutes before your actual planned colonoscopy "start" time to allow for registration and admission to the Southwest Endoscopy Center, changing into a medical gown in a private preparation area, a preprocedure nursing assessment, placement of an IV line to allow administration of sedatives during your procedure, and a presedation physician assessment of your general health status and airway (mouth, throat and neck). Your family member or a friend is welcome to stay with you during this time. When all preprocedure preparations have been completed you will be taken by stretcher to the procedure room (where family members may not be with you), where a variety of monitoring devices (electrocardiographic skin electrodes, blood pressure cuff, finger oxygen sensor) will be placed. Either a nasal tube or an oxygen mask will be secured into position to provide oxygen during the procedure and allow for monitoring of exhaled carbon dioxide levels.
Once everything is ready and your gastroenterologist is in the room, a nurse anesthetist will administer a sedative under the doctor's direction. A second nurse or technician will assist the doctor. Colonoscopy usually takes about 15 minutes of actual instrument-in-the-body procedure time, though technically demanding procedures may occasionally take twice this long. Most patients sleep through their procedure and begin to awaken shortly after it is completed, prior to being taken by stretcher back to their preparation area, where they are monitored for a few minutes during recovery from sedation. While the procedure itself is typically painless, some abdominal discomfort and distension from the air used to hold the colon open for examination is common. This sensation usually subsides in a few minutes with some passing of odorless gas, which we require of our patients, regardless of usual social considerations.
Most of our patients are ready to be discharged home about 20 minutes after the completion of their procedure, after reviewing their written procedure report and any necessary instructions with our nursing staff.
|
I am worried about the idea of being sedated. How do you do this and how safe is it? (click for more information)
How do you clean the instrument before you use it on me? (click for more information)
How will I feel after its done? What can I do the rest of the day?
Most patients feel a little bloated, relaxed, and relieved. Many are hungry and anxious to find some food. We recommend that you not drive, eat a light meal to start with, and take it easy for a few hours. Many patients can then resume most of their activities right away, though driving should be restricted until the following day. You should expect to resume all of your normal activities the next day.
This depends on your underlying bowel habit and your diet after the procedure. Most patients return to normal bowel function within 1-3 days.
What does a normal colon look like during colonoscopy?
|
 |
| Normal colon |
|
|
Photograph of normal descending colon. Complete cleansing of the colon is critical to ensure an optimal examination. This photograph shows the results of a good quality bowel "prep" resulting from Digestive Health's preferred split dose oral electrolyte lavage standard colon cleanse.
|
|
What is a polyp, and why should I care if I have one?
Polyps are common growths which develop on the interior lining of the colon. The term "polyp" is commonly used to describe colon lesions which are often raised growths projecting from the colon surface but may also be elevated and flat or even depressed in shape. Some polyps, particularly those known as adenomas or adenomatous polyps, develop as a result of genetic mutations. While such polyps are benign (not malignant or cancerous) they have the potential to acquire additional mutations over time and become malignant (cancerous). The process of cancerous change is typically slow (5-10 years) and only occurs in a small minority of at-risk polyps. Generally, polyps and the early cancers resulting from them cause no symptoms, though occasionally such growths will bleed. Once a cancer invades the wall of the colon it may spread to regional lymph nodes and distant organs such as the liver, rendering it essentially incurable.
Polyps are generally removed as soon as they are detected during the performance of a colonoscopy, to prevent progression to cancer.
|
 |
| Pedunculated tubulovillous adenoma with high grade dysplasia |
|
|
Photograph of a pedunculated (mushroom-shaped head on a stalk) polyp with advanced premalignant changes.
In this case the abnormal tissue at the head of the polyp is attached to the colon wall with a broad stalk. The stalk tissue itself does contain potentially premalignant tissue changes. This polyp was fully removed at the time of colonoscopy at the Southwest Endoscopy Center with a cautery snare.
|
 |
| Nonpolypoid superficial elevated adenoma |
|
|
Photograph of a nonpolypoid superficial elevated (flat-shaped, elevated) lesion.
This growth was also fully removed (endoscopic mucosal resection) at the time of colonoscopy at the Southwest Endoscopy Center
|
If I have a polyp, do I have to come back to have it removed?
Most polyps and flat lesions are removed completely at the time of colonoscopy. If not, a repeat visit may be needed to complete removal, or to closely monitor the area of removal for recurrence. Surveillance colonoscopy is recommended at an interval prescribed by your doctor to allow for detection of any recurrent or new polyps before they become a threat to your health. Most often, surveillance examinations are recommended at 5 year intervals, though a 3 year initial repeat examination may be advised in the case of multiple polyps or polyps which are large or high grade. In some cases a repeat examination after a few months may be recommended, typically after removal of large flat polyps.
|
I have read about flat lesions, and that they can be missed by a colonoscopy. Do you know about this?
|
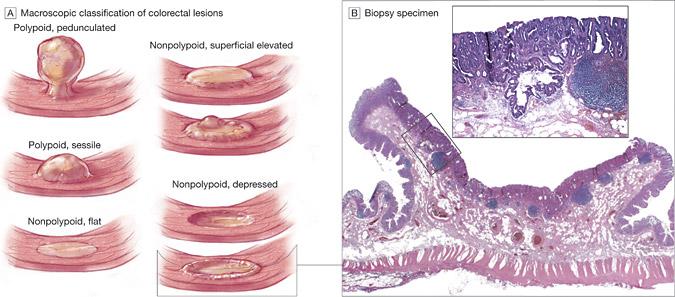
From: Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults. Roy M. Soetikno, MD, MS; Tonya Kaltenbach, MD, MS; Robert V. Rouse, MD; Walter Park, MD; Anamika Maheshwari, MD; Tohru Sato, MD; Suzanne Matsui, MD; Shai Friedland, MD, MS. JAMA. 2008;299(9):1027-1035. Used with permission.
As shown above in the illustration from a March 2008 article in the Journal of the American Medical Association, potentially premalignant growths (adenomas) are seen in a variety of shapes and sizes. The most elevated lesions are easiest to detect and remove. Elevated lesions are called polyps, whether they are mushroom-shaped (pedunculated type) or form a more broadly based flatter lump (sessile type) on the colon lining. Flat adenomas and depressed adenomas (nonpolypoid colorectal neoplasms (NP-CRN) are less common, carry greater risk of malignant transformation over time than elevated polyps, and are more difficult to detect. With high quality colonoscopy however, these flat adenomas (nonpolypoid colorectal neoplasms (NP-CRN) can be detected and removed.
Colonoscopy by an experienced gastroenterologist, after a high quality cleansing bowel preparation, is the best way to catch these growths. In some cases a dye may be sprayed over the lesion to help visualize the full extent of the growth (chromoendoscopy). We are very aware of these lesions at the Southwest Endoscopy Center and we take great care to detect them during every examination. As we discuss below however, no test is 100% accurate for finding flat adenomas or other lesions within the colon.
|
What is colon cancer, and what does it look like during a colonoscopy?
|
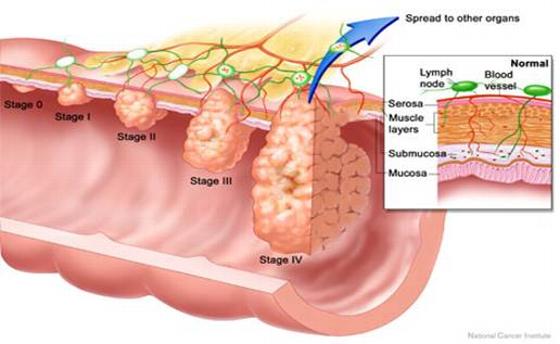 |
| National Cancer Institute graphic showing the stages of colon cancer progression |
|
|
Polyps and early colon cancers usually do not cause symptoms. The good news is that in most cases early colon cancers are quite detectable by colonoscopy. Early cancers are also usually curable. The necessary treatment may involve colonoscopy alone (with removal of a cancer-containing polyp), surgical removal of the cancer and adjacent section of the colon, and sometimes, radiation and chemotherapy.
|
 |
| Early colon cancer |
|
|
|
Photograph of an early colon cancer (extending from six o'clock to about 9 o'clock along the thickened fold) in the ascending colon. This patient underwent surgical removal of the affected section of his colon, but because the cancer was early stage, no chemotherapy was needed. He is cancer-free and feeling fine eight years after diagnosis and treatment.
Advanced cancers have already spread to distant lymph nodes or organs, such as the liver. Tumors which have spread in this manner often cannot be cured, but tumor progression can be effectively slowed in many cases with chemotherapy. Prevention of colon cancer, by the detection and removal of potentially premalignant polyps, is the best approach. Failing prevention, the detection of colon cancer at an early and curable stage is the key to an optimal medical outcome.
|
 |
| Advanced colon cancer |
|
|
|
Photograph of a large colon cancer obstructing the colon in its upper portion (cecum). In this case the abnormal tissue is shown in the center of the photograph, where it completely fills the normal hollow tube. This patient needed surgery and chemotherapy, though he is feeling well and free of evident cancer over 10 years after his diagnosis.
|
I think I have hemorrhoids. Can they be treated at the time of my colonoscopy?
Hemorrhoids are engorged veins that may extend from the junction of the rectum and interior anus through the anal canal to the external anus. Hemorrhoids are common. While they frequently cause symptoms of minor bleeding, pressure discomfort, itching and protrusion of tissue during or following a bowel movement, they may cause no symptoms at all. Minor hemorrhoidal symptoms may improve with a concerted effort to take in additional dietary fiber. A good product is Kellogg's� All-Bran Bran Buds� cereal. In many cases additional treatments are helpful. Surgery (hemorrhoidectomy) is generally reserved for the most severe cases which cannot be managed with simpler means.
|
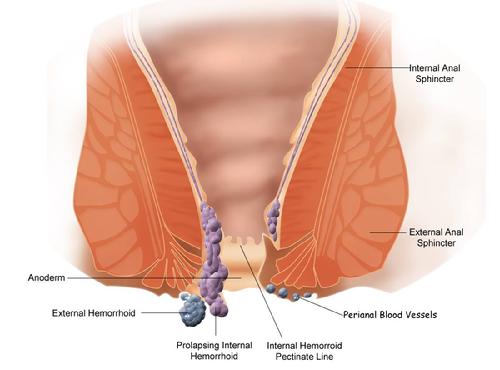 |
| Hemorrhoid anatomy (from Wikipedia) |
|
|
Two treatments can be performed at Digestive Health or Mercy Regional Medical Center while you are sedated for colonoscopy:
Infrared coagulation (IRC)
IRC uses an infrared light source to heat (photocoagulate) pea-sized dots of skin in the rectum just above the hemorrhoid. Typically, 6-12 coagulations are performed in a session, moving around the circumference of the lower rectum. This treatment is painless when performed under sedation immediately following the completion of your colonoscopy. Recovery is usually immediate. A mild aching discomfort occasionally follows treatment for up to an hour. As the healing process begins to occur in the days following treatment some minor bleeding is typical, as the coagulated tissue begins to slough. This treatment works in part because the healing process leads to beneficial scar tissue formation which "tacks" the loose hemorrhoidal tissues to the underlying rectal wall and reduces blood flow into the remaining hemorrhoidal channels. IRC rarely leads to significant complications, and can be repeated if necessary. It is the procedure of choice for low grade hemorrhoids.
Band ligation
High grade hemorrhoids, particularly those which protrude, or prolapse through the anal canal, may not be good candidates for treatment with IRC, but often respond well to hemorrhoidal band ligation. This treatment can also be performed under sedation immediately following completion of colonoscopy. The doctor uses a device known as a ligator inside the rectum (above the border of sensitive anal canal skin) to suction the loose tissue at the base of the hemorrhoid into a small cup around which a tiny rubber band is placed, leaving a small firm ball of tissue about the size of a large blueberry. One to three bands may be placed during a treatment session. While the performance of the banding itself is painless under sedation, it is not unusual for patients to awaken with an aching anorectal discomfort. Usually this subsides over the course of an hour or so, but occasionally it will require treatment with sitzbaths, pain medication and suppositories for a day or more. The healing process involves clot formation (thrombosis) in the affected hemorrhoid and sloughing of the banded tissue over the course of a week or so. While this is often a painless process, in some cases pain, protrusion of the thrombosed hemorrhoids and bleeding can be significant problems. Rare but potentially life-threatening infections have been reported after banding, so it is important to keep your doctor informed if you are having any persistent or worsening symptom such as pain, particularly in the presence of fever or chills, after this treatment. Band ligation may also be safely repeated, if needed.
In June 2011 we added what we believe is a "kinder and gentler" form of band ligation, the CRH O'Regan System treatment, to the procedures available at the Southwest Endoscopy Center. This form of ligation is also performed in our clinic, allowing periodic retreatment at 2 week intervals until hemorrhoidal symptoms resolve.
If you are experiencing hemorrhoidal symptoms and want your gastroenterologist to consider performing one of these treatments please discuss this with us before your procedure.
|
 |
| Hemorrhoids |
|
|
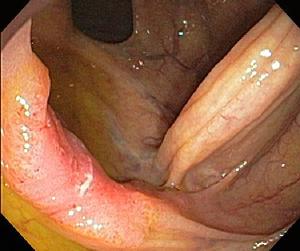
This view shows internal hemorrhoids in a "retroverted" view, in which the flexible tip of the colonoscope is bent into a 180 degree "u-turn" showing the junction of the interior anus and rectum from above. The instrument is black. The hemorrhoids are bulging blue structures adjacent to the instrument. This patient was treated with band ligation.
|
Hemorrhoid Treatment Aftercare
I heard that colonoscopy can miss abnormalities and cause complications that sometimes even require surgery. Is that true? Why should I risk that if I feel fine?
While colonoscopy provides the very important health benefits of early cancer detection and cancer prevention, there are potential risks of having the procedure performed, even when it is properly performed by an expert who is using proper technique and appropriate caution and care. Fortunately, for most patients these risks are far outweighed by the benefits. Doing nothing and taking your chances with colon cancer is itself a risky proposition, and far more people would be harmed by simply hoping for the best and avoiding colon cancer screening-prevention measures than by undergoing colonoscopy by an experienced gastroenterologist at a facility providing this procedure on a routine basis in a safe and effective fashion.
It is important for you to feel that this is the right procedure for you before proceeding. Your primary care provider is one of your best resources for helping you with the decision to undergo colonoscopy. If your primary care provider is 50 years of age or older, the chances are that he or she has already undergone colonoscopy, and he or she may be willing to share their personal experience in addition to their medical advice. All three of the Digestive Health gastroenterologists who perform colonoscopy at the Southwest Endoscopy Center have themselves had colonoscopies performed on them at this facility.
Risks
The most common and important risks of colonoscopy are the risk of missing something, the risk of a perforation, the risk of bleeding, the risk of diverticulitis, the risk of injury to the spleen, and the risk of heart or lung problems related to sedation. Colonoscopy performed by an experienced gastroenterologist is the most accurate means of detecting abnormalities such as colon cancer or colon polyps, but no test is 100% accurate in this regard.
The Southwest Endoscopy Center is committed to minimizing the risk of complications which result from colonoscopy. To that end, we participate in a prestigious ongoing multicenter endoscopic outcomes research project known as CORI. One of our projects has been a study designed to determine the frequency with which complications from colonoscopy actually lead to hospitalization. Perhaps surprisingly, the medical literature does not accurately define procedural complication rates, partly because complications are fairly uncommon events, making them difficult to tally, and partly because they are often "underreported" in a study format. In some cases, for example, the doctor who performed the colonoscopy might not even be aware that the patient was hospitalized at a different facility in a different town for treatment of a complication.
In this colonoscopy complications study, our patients who agreed to participate were contacted by University of Washington researchers at 7 and 30 days after their colonoscopy, at which times they were questioned regarding any health problems that might be related to their procedure. The results of this study were published in October 2009 in Clinical Gastroenterology and Hepatology. Digestive Health colonoscopy patients made up over 1,000 of the 21,375 cases included in this report. In these patients, the rates of problems following colonoscopy leading to hospitalization were:
-
bleeding requiring hospitalization (1.5 per 1000 exams)
-
bleeding requiring transfusion (0.8 per 1000 exams)
-
perforation (0.16 per 1000 exams)
-
diverticulitis (0.9 per 1000 exams)
-
diverticulitis requiring hospitalization (0.3 per 1000 exams)
-
postpolypectomy syndrome (0.1 per 1000 exams)
-
hospitalization for any colonoscopy-related cause (0.2 per 1000 exams)
In most cases, the risks of a serious complication of colonoscopy are easily outweighed by the benefits of cancer prevention and early cancer detection (detection when cure is possible). While events such as perforations are uncommon, they do occur occasionally in the context of a properly and carefully performed colonoscopy. When complications do occur early diagnosis is important to an optimal outcome. If you are having any unexpected symptoms after an examination, such as bleeding, increasing abdominal pain or fever, it is important to contact Digestive Health immediately and confer with your gastroenterologist or with the doctor who is providing coverage if your gastroenterologist is not available (see Emergencies).
Perforations and similar serious injuries may require surgery for treatment. While sending an otherwise healthy patient for an operation because of a colonoscopy complication is always a very difficult matter, doctors and family members of individuals who have succumbed to colon cancer know that the risk of a very uncommon and fixable problem is much easier to bear than the risk of missing an opportunity to prevent a relatively common and often fatal disease.
I had a colonoscopy this morning and now I have chills, fever and body aches. What is going on and what should I do?
These symptoms are not expected and should be reported immediately to your physician. If you also have abdominal pain or tenderness, an endoscopic complication such as perforation must be assumed to have occurred, until proven otherwise. Early diagnosis and treatment is key to achieving the best outcome. If you have no abdominal symptoms your fever, chills and muscle aches may be due to the sedative administered for your procedure, particularly if you received propofol. The FDA and CDC have investigated clusters of propofol-associated fever from around the country, as discussed here. Evaluation and treatment for bacterial sepsis is recommended if this problem is suspected.
FDA Alert of June 2007
I have a heart problem, and I need antibiotics before dental procedures and surgery. Do I need antibiotics for colonoscopy?
No. For decades we have administered IV or oral antibiotics prior to performing some colonoscopy procedures, but practices have changed. In April 2007 the American Heart Association updated its prior guidelines, which had been in place since 1997. The new guidelines state that "the administration of prophylactic antibiotics solely to prevent endocarditis is not recommended for patients who undergo GU or GI tract procedures, including diagnostic esophagogastroduodenoscopy and colonoscopy." The guidelines, which were published in the April 2007 edition of the journal Circulation, can be viewed here.
I have an artificial joint. My orthopedic surgeon said I need antibiotics for colonoscopy. Is this true?
No. The American Society for Gastrointestinal Endoscopy (ASGE), has concluded that antibiotic prophylaxis for patients with prosthetic joints is not recommended. If your surgeon advises you to take antibiotics anyway before and/or after your procedure, he or she may choose to provide you with a prescription for the agent of their choice. Click here to review the 2008 ASGE recommendations in their entirety.
When do I get my results?
Your full procedure report will be completed by your gastroenterologist and provided to you by our nursing staff, who will review your findings with your at the time of discharge. If any tissue (biopsies, polyps) was removed during your examination it will be forwarded to Mercy Regional Medical Center for examination by a pathologist. Your gastroenterologist will contact you with further information about these specimens, typically in 7-14 days. A copy of these reports will be provided to your referring provider and to any other doctor or health care provider you choose, at your direction.
I had a screening colonoscopy and the doctor found a "large" polyp but did not remove it. Now I have to come back for another colonoscopy to have it removed. Why didn't the doctor remove it during my screening exam?
Polyps are commonly found and removed during screening colonoscopy. At the Southwest Endoscopy Center we remove at least one polyp in over half of the screening colonoscopies we perform. Over 80% of these polyps are small (defined as < 10 mm). While we also remove the majority of large polyps that we encounter at the time of a screening exam, some polyps may be left in place to be removed at a later date, either at the time of another colonoscopy or during a laparoscopic or open surgical procedure.
If the doctor, based on the size, shape, location or other characteristics of the polyp, decides that special advanced endoscopic or operative surgical techniques are necessary, removal will be deferred. Not all experienced gastroenterologists perform certain advanced techniques such as EMR (endoscopic mucosal resection) that may be necessary to safely and effectively remove these polyps. In those instances the doctor may consider referral to another specialist, locally or at a tertiary referral center. In some cases additional staff or equipment may be necessary for optimal management. The risks associated with removal of a large polyp can be much greater than the risks of conventional polyp removal. The doctor may choose to more specifically discuss the options of higher risk colonoscopy, and the probability that multiple follow up examinations over the course of several years may be necessary to ensure that the growth has been successfully eradicated, as well as the alternative option of surgical removal, prior to performing an EMR. In some cases biopsies may be performed, and the results may be used to guide treatment. In many cases in which a polyp is identified but not removed the location will be marked with a tattoo.
Will my insurance pay if I have to have another colonoscopy to remove a polyp the doctor didn't take out the first time?
Yes. Insurance covers medically necessary care. Be aware however that a colonoscopy performed to remove a known polyp is not a "screening" colonoscopy. The waiver of cost-sharing (deductible and copay) that is common under the Affordable Care Act for screening colonoscopies does not apply to a "therapeutic" procedure.
When do I need to have another exam?
Your doctor will let you know when another colonoscopy should be planned, based on your findings, your family history, and other factors which may be important in your case. The quality of bowel cleansing and the size, shape, number and microscopic characteristics of any polyps found factor into our recommendations, which in most cases follow these guidelines.
We hope that this information helps you put the risks and benefits of colonoscopy in perspective.
Your gastroenterologist will be happy to talk with you further about this before your procedure.
Please don't hesitate to share your questions and concerns.
|
|